

Mills & Co Provide Parents No Comfort on Potential COVID Vaccine Mandate for School
On October 20, the CDC’s Advisory Committee on Immunization Practices (ACIP), to which Maine CDC Director Dr. Nirav Shah is a recent addition, unanimously voted to add COVID-19 vaccines to the recommended schedule of childhood immunizations.
The vote was unprecedented. It was the first time in history that a vaccine product under Emergency Use Authorization (EUA) was added to the CDC’s national recommended immunization schedule. By doing so, Shah and the rest of ACIP members gave Pfizer and other pharmaceutical companies protection from liability for injury and death that result from Americans (young and old) taking their COVID-19 products, under the National Childhood Vaccine Injury Act of 1986. Today, these companies are covered from liability in that such products are considered temporary, emergency “countermeasures” under the PREP Act.
If President Biden and Xavier Becerra, Secretary of Health and Human Services, did not extend the federal public health emergency designation on October 13, the authorization to distribute COVID-19 vaccines under EUA to children would vanish. Even though President Biden recently declared that “the pandemic is over” on the TV program 60 Minutes, promoting these products to children and parents has taken precedence.
Many states look to the CDC’s recommended schedule as a benchmark for their own lists of mandatory vaccinations to attend public school. Does Dr. Shah’s support for adding these emergency-use products to the national immunization schedule mean that he would support a similar move on the Maine state level?
In a normal season, concerned parents and voters would normally look to the chief executive to provide clear guidance. Unfortunately for Mainers, its campaign season, and Governor Janet Mills is running for re-election. Those looking for unambiguous information from the administration in Augusta are out of luck.
When asked during an October 24 debate “lightning round,” about whether she would support adding COVID-19 injections to the state schedule, Mills responded, “No, not at this time.”
Translation: not before the election.
Her opponent, former Governor Paul LePage, responded with an unequivocal, “No.”
In another debate on October 27, Mills explained that she would not pursue a K-12 student mandate while the COVID-19 vaccines were still under EUA, even though she had no problem firing healthcare and emergency management workers if they didn’t take the EUA product a year ago.
Here's Gov. Mills on vax mandates for school kids Monday vs Thursday.
— Steve Robinson (@BigSteve207) October 28, 2022
Different answers, but she's still leaving the door open to, perhaps after the election, mandate that school children get the injections in order to attend Maine public schools. pic.twitter.com/IJF1yjQAdH
Difficult to see how these two different answers would give parents of the majority unvaccinated school-aged Maine children more peace of mind.
Other incumbent governors running today have given similarly questionable answers on this topic as well. In a recent debate, New York Governor Kathy Hochul said “we’re not talking about mandating a vaccine for children in school at this time,” noting that the Legislature could take up that question next year. Hochul did not comment on how she would handle a bill to that effect.
Answers like those offered by Mills and Hochul are unlikely to comfort parents worried about a mandate in the near future. In Maine, children who are considered “fully vaccinated” make up less than half of the school-age population. Among those under age 5, less than 7 percent have received initial doses. Clearly, there is trepidation among parents—even those who have received the shots themselves—to allow their children to get them too.
If Maine’s Department of Health and Human Services (DHHS) and Department of Education (DOE) are successful in pursuing a mandate, it would result in tens of thousands of Maine K-12 students being kicked out of their school at present, including charter and private schools. This move would likely result in a mass exodus of families from the public education system, and likely the state itself.
Only 44.29% of children ages 5-11 have received a final dose of the COVID-19 vaccine in Maine.
— Maine Policy Institute (@MainePolicy) October 25, 2022
Only 71.92% ages 12-19 have received a final dose.
A vaccine mandate amounts to an estimated 87,766 school-eligible kids kicked out of public schools.#mepolitics https://t.co/oGzG616rz4
This would make Shah and Mills more radical than national public health communicators like former Surgeon General Jerome Adams and former FDA head Scott Gottlieb. While the Mills administration had dutifully followed federal guidance for nearly all of the pandemic, their current policy mandating COVID-19 shots for healthcare workers directly contradicts CDC’s latest iteration. They are clearly willing to be more radical than the feds; could mandatory childhood vaccination be next?
What would be the point of a mandate like this, anyway? Informed, objective analyses of COVID-19 vaccines for children show very low absolute benefit, given that the young are very rarely hospitalized for COVID. Plain and simple, American society should not regard these products as “routine” for children.
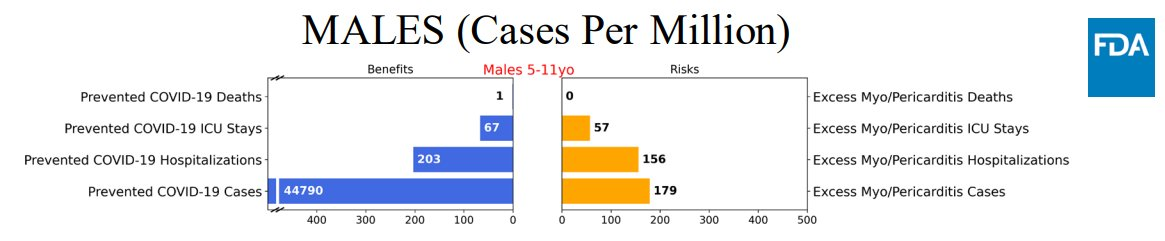
Even an expert FDA advisor, Dr. Hong Yang, Senior Advisor for Risk-Benefit Assessment at the FDA’s Office of Biostatistics and Epidemiology, recognized this out of balance risk-benefit ratio in a presentation to the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) over a year ago. The most striking slide from Dr. Yang’s analysis (below) showed a prediction that vaccinating males aged 5 to 11 would prevent 67 ICU stays and 203 hospitalizations for COVID-19 per one million boys, but would also result in 57 ICU visits and 156 hospital stays for vaccine-induced myocarditis. This analysis only considered myocarditis and heart-related risks post-vaccination, not other potential safety risks. That alone should have given national advisors pause to promote giving these products to children.
As Dr. Vinay Prasad, professor at the University of California-San Francisco, explained in a recent article that COVID-19 vaccines are very different from the others present on the CDC’s schedule. The new shots have not been shown to reduce infection and transmission of the disease they target, nor have they undergone many years of trials to clearly define safety and efficacy, as other CDC-recommended vaccines have. As he notes,
“Measles can be a devastating childhood illness, but vaccination provides durable, sterilizing immunity…Covid-19 vaccines, as millions have learned, do not prevent you from getting Covid-19. Right now the CDC director Rochelle Walensky has Covid, despite being boosted with the bivalent booster just one month ago.”
— Vinay Prasad, MD, MPH
Data presented in a September 2022 letter to the editors of the New England Journal of Medicine show that the protection offered by COVID-19 vaccination against infection for children wanes precipitously, as is the case for adults as well. The two graphs below show that children in the study who had been previously infected with the virus that causes COVID-19 (left) retained relatively strong immunity against successive infection, falling to between 45 and 60 percent after five months, for as long as 15 months after recovery. Whereas, for those children who received a COVID-19 vaccine (right), effectiveness against infection fell to zero after about six months.

As for safety, the greatest recognized safety risk from these new injections have been types of heart muscle inflammation known as myocarditis or pericarditis. A peer-reviewed study published in the New England Journal of Medicine in December 2021 which looked at more than 2.5 million COVID-vaccinated health care workers found that males between ages 16 and 29 were at the highest risk of myocarditis after vaccination. This study found that the young male cohort experienced myocarditis at a rate of 10.69 cases per 100,000, or 1-in-9,354.
A preprint study posted in March of 2022 found that “Young males infected with the virus are up 6 times more likely to develop myocarditis as those who have received the vaccine.” Authors estimate that these heart issues affect as many as 1-in-2,222 vaccinated males aged from 12 to 17. COVID-19 vaccination carries clear for young males, with very little benefit for children overall. Any mandate for this age group to receive it is gravely misguided.
Maine media should continue to press Gov. Mills on this question. Since, given her latest statement, it is evidently still up for debate within her administration. Do Mills and her own CDC director, who she praises so often, differ that much? Clearly, these shots do not benefit college-aged students, yet the administration has not urged abolition of COVID vaccine mandates to attend university and community college. What reassurance do parents of K-12 students have that they also won’t be forced to take these shots in order to attend school?
Dr. Shah’s vote and statements in support of adding the shots to the national schedule—as well as Mills’ equivocation on the issue—should prompt parents, as well as Maine legislators, to resist any attempt to add these investigational, emergency-use products to Maine’s immunization schedule, lest tens of thousands of children be unnecessarily robbed of their futures.