
Covid Catastrophe is a seven part series examining the history of the COVID-19 pandemic, its impact on Maine and what data policymakers used to lock down society and centrally-plan our economy. Check back tomorrow for Part V.
Maine recorded its first case of COVID-19 on March 12. During the week of March 15, Governor Mills declared a Civil State of Emergency, recommending that schools close, gatherings of more than 50 people be cancelled or postponed, restaurants and bars close for two weeks, and elective medical procedures be delayed. This early order also designated which businesses would be considered “essential” and which would be considered “non-essential” by the state. This delineation would prove to be the greatest hurdle for many businesses, merely to attempt to make ends meet under the governor’s new rules.
By the end of March, Governor Mills had ordered all non-essential businesses to close any public-facing operations and issued the “Stay Healthy At Home” order, banning all non-essential travel. The few public spaces deemed integral to public health, like grocery stores, pharmacies, repair shops, etc., were ordered to comply with state rules requiring physical separation and frequent sanitation of spaces. Restaurants could only offer take-out or delivery service, for example. Shortly after, state officials released the phased “Restarting Maine’s Economy” plan, outlining how and when certain industries could expect to reopen. Heather Johnson, the Commissioner of Economic and Community Development, issued checklists for each sector to follow in order to reopen within the phased plan.
Two days before the governor announced her plan, Maine Policy Institute published and presented a proposal to guide the administration’s decisions, stressing the need for flexibility, balance, and trust in people to make smart decisions for the health of their communities. Over 5,500 Mainers signed on to Maine Policy’s recommendations. Despite the resounding message from industry leaders, workers, and families across the state, the Mills administration released its phased-in reopening plan that, from the outset, arbitrarily picked winners and losers in the economy.
Unfortunately, the phased reopening left many businesses out of the loop and unable to attempt to serve customers and pay employees while operating at a limited capacity. The Mills administration could have issued health and safety guidance for businesses to that end, but instead mandated all but those deemed “essential” to close. To date, Maine Policy has compiled an unofficial list of the businesses that have reported permanent closure, through local broadcast media or social media, due to the state response to the coronavirus. At time of publication, that list exceeds 75 businesses across Maine, not including the numerous cancelled fairs and festivals on which many towns and local businesses rely for tourism-related revenue. The true number of permanently closed businesses won’t be realized until 2021 business license data become available.
In mid-April, Maine experienced its highest number of daily COVID-19 deaths. Thirty-two Mainers succumbed to the virus between April 13 and April 27, one quarter of the state’s total deaths as of late July. The state began to include “possible cases” as part of the totals during that time, counting not only confirmed positive tests, but also close contacts of individuals who tested positive, as well as those with a positive antibody test and some symptoms. At the bottom of its COVID-19 data dashboard webpage, the Maine CDC outlines the specific factors it considers when determining possible cases.
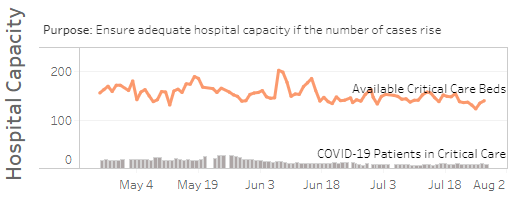
Since the beginning of the outbreak, Maine state officials largely followed the advice and guidance of the federal CDC. Maine state officials and the White House used the University of Washington IHME model to try to anticipate the spread of the new virus. In mid-March, just before Governor Mills declared the state of emergency, the U.S. Surgeon General called on states to delay elective medical procedures to attempt to conserve personal protective equipment (PPE) and hospital capacity in the event of exponential growth in serious coronavirus cases. In the early weeks of this pandemic, state and federal officials focused on the risk of an overburdened healthcare system, as many had seen in reports from Italy the month before, encouraging the public to do as much as possible to “flatten the curve.”
Critical Care Capacity in Maine
Later in the spring, we would hear about hospital systems across the country, including in Maine, that had to furlough, lay off, or cut hours of nurses, practitioners, and other hospital employees, due to the loss of revenue from postponed procedures. While this sort of unintended consequence appeared relatively early, the true health consequences of delaying procedures unrelated to COVID-19 are likely to be unrealized for many months or years. A report published in the National Institutes of Health (NIH) Public Health Emergency COVID-19 Initiative cites an estimate that 91% of surgeries in the US are considered elective and mentions that, “Delays in surgery have been shown to result in higher rates of surgical site infections, leading to increased costs ranging from $7,000 to $17,000 for coronary artery bypass graft and colon and lung resections.” The report further states:
“The medical consequences of surgical delays will likely manifest in increased costs to the health care system via treatment of more advanced disease, often requiring more intense and more costly treatment. For example, disease progression in breast, colorectal, and lung cancer is associated with an annual increase of $50,000 per case.”
Patients who had to postpone their biopsy or cancer screening delayed a potentially earlier diagnosis crucial to ensuring recovery. We are beginning to see that the effects of government overreaction to the pandemic contributed to worse health care outcomes than what the virus could have reaped on its own.