
There has been no shortage of research into the risk factors that contribute to contacting SARS-CoV-2, and to sever COVID-19 illness from infection, since the world learned of a novel coronavirus emerging from Wuhan, China in December 2019.
Published in April 2021, a Kaiser Permanente study of more than 50,000 people found that the highest risk factors of COVID-19 illness for the overall population are advanced age (older than 60), a recent organ transplant, and physical inactivity. Even greater than underlying health conditions like hypertension or diabetes, “patients who were consistently inactive had 1.73-fold greater odds of ICU admission than patients who were consistently active.”
While older age carries greater risks related to COVID-19, children thankfully face very low risk of contracting severe illness. Unfortunately, however, youth have borne the brunt of single-minded COVID-19 policymaking, leading to decreased health and fitness over the course of the pandemic.
A recent study from the US Centers for Disease Control and Prevention (CDC) found that rates of obesity among American youth, as measured by body-mass index (BMI), rose sharply during the pandemic compared to the world before COVID-19.
Among more than 430,000 people between the ages of 2 and 19, the CDC recorded that “the monthly rate of BMI increase nearly doubled during the COVID-19 pandemic period compared with that during the pre-pandemic period.” In August 2019, they estimated that 19.3% of this group were obese. One year later, that estimate had risen to 22.4%. This amounts to a 16% increase in overall rates of youth obesity during the height of pandemic school closures and societal shutdowns. Among 5 to 11 year-olds, the rate of obesity increased by 26%.
Tragically, these disparities were most pronounced among younger age groups, as well as among those already experiencing obesity. People who are obese as children are vastly more likely to be obese in adulthood, with greater potential to develop other chronic health problems.
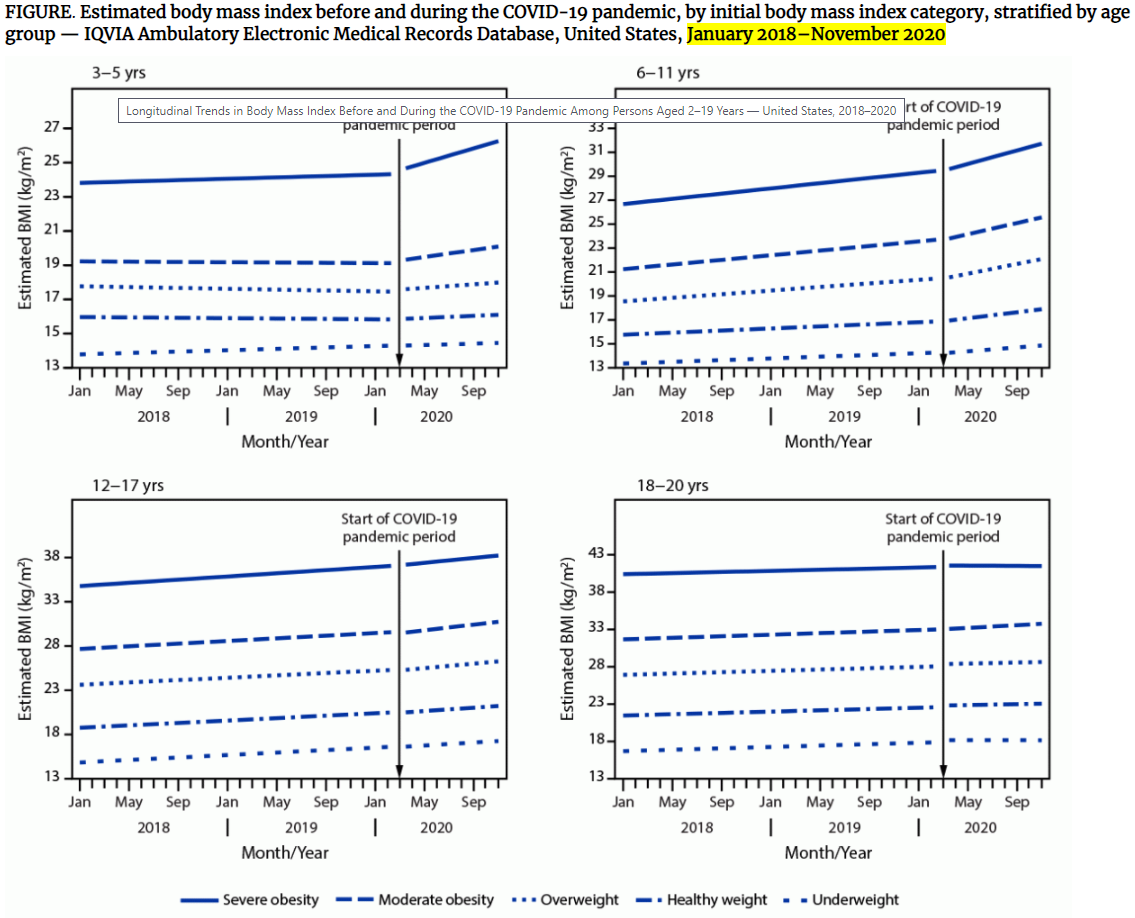
Source: Centers of Disease Control and Prevention
A 2020 survey of Canadian youth also reported lower levels of physical activity, less time spent outside, more sedentary behaviors, and more sleep than before the pandemic. Unfortunately, this shows that children were challenged to maintain healthy levels of physical activity during lockdowns. Combined with noted increases in depression and the substantial reduction in public activities, the average child was at a disadvantage in forming a healthier lifestyle during that time.
According to a narrow “COVID-19 and Youth” dataset released by the Maine CDC on September 20, we know that among more than 26,000 confirmed or probable “cases” of COVID-19 in Mainers under age 25, fewer than 60 resulted in hospitalization. These numbers are not adjusted for underlying health status, nor to account for potential overcounting, which a recent exposé by The Atlantic noted could be at least a third. More than half of these recorded hospitalizations are among Mainers 18 and over. Only seven Maine children aged 5 to 14, or 0.09%, have been hospitalized with COVID-19.
Overall, Mainers aged 0-19 face a 0.22% chance of becoming hospitalized with COVID-19, given a confirmed or probable case. While they account for more than 20% of the statewide population, and about the same proportion of total cases, they account for 0.1% of COVID-related fatalities. Weighted for their share of the population, the risk of death from COVID-19 for Mainers under 20 is 0.005%: 1-in-20,000 odds. This factor has been nearly unchanged since the beginning of the pandemic, well before vaccines were available for a portion of this group.
Looking at data from the US CDC, also not adjusted for health status, the COVID-19 case-fatality rate (CFR), which measures how likely one is to die after being deemed a confirmed or probable case, is extremely low for children in the US. Those under 12 face a CFR of 0.012% and for those under 40, the CFR is 0.07%.
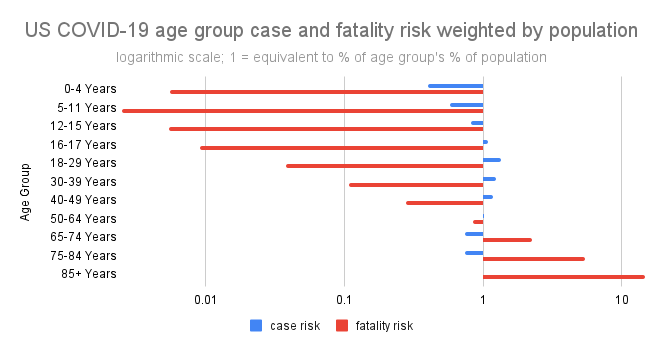
Source: Maine Policy Analysis of Maine CDC data, September 29, 2021
Data show that 5-11 year-olds experience the lowest risks from COVID of any single age group tracked by the CDC, less than 1/200 that of an average American. Add to this the fact that children under 12 are much less likely to even contract the virus; they make up 14.7% of the population but only 7.4% of COVID cases. Even if they do catch it, they are much more likely to be asymptomatic, which may account for some underrepresentation of the group in case data; one is less likely to be tested if they are not sick.
In addition, asymptomatic spread of SARS-CoV-2 was shown to be very low in an extensive meta-analysis covering more than 77,000 participants published in the Journal of the American Medical Association (JAMA) in December 2020. Have our reactions to this virus caused more harm to young people than the pathogen itself?
Sadly, there have been some severe cases of COVID-19 in youth, with instances of a serious condition called multisystem inflammatory syndrome (MIS-C). Another JAMA study published this June looked at the incidence of the condition in COVID-19 patients. It estimated that although slightly higher in cases among children ages 6 to 10, the condition resulting from COVID-19 is still quite rare: between about one-in-130,000 among that age group, to about one-in-200,000 for all patients.
So-called “long COVID” has been seen in children as well, where the recovered still experience lingering after-effects from their infection, but a researchers from King’s College of London recently found that more than 95% of young patients four weeks after infection, and more than 98% eight weeks afterwards, no longer had symptoms.
Just in the past week, multiple schools in Maine announced they were closing and again moving to remote instruction in response to rising positive SARS-CoV-2 tests among students. Old Town High School is even implementing a three-strike policy for students who violate the universal mask-wearing policy. In mid-September, half of the Bangor High School football team was in mandatory quarantine, sitting out of games and practice, and staying home from school for two weeks. This was required not because they were necessarily sick, but because the district policy for “close contacts” of those who test positive follows the CDC policy.
Continuing to try to shield the young from a ubiquitous respiratory virus, for which they experience minimal risk, in order to protect adults (the vast majority of whom are vaccinated) is an inexcusably ignorant response nearly two years into this saga.
State and local leaders must recognize this folly as soon as possible, and prioritize actual health for the youth: exercise, good diet, interacting with peers, and pursuing an education uninhibited. They should be free to finally catch up to what adults have taken away from them.