
Reports across Maine over the last month have detailed the several healthcare facilities forced to curtail services because of staffing shortages. While this rationing of care is due in part to issues which have plagued Maine’s economy for years, as Governor Janet Mills contends, it also comes in response to Mills’ mandate that all healthcare workers be “fully vaccinated” for COVID-19 by October 29. There is little question that this long-term problem has been exacerbated by her recent mandate.
Then, in true form, she offered a plan to fix the problem that she helped create. On Monday, the governor held a press conference to shift public focus from the numerous healthcare workers she is forcing to be fired to emphasize a plan to grow the state’s crucial healthcare workforce. Truth be told, the $14 million for four programs she announced were passed into law back in July as a part of LD 1733, also known as the “Maine Jobs and Recovery Plan,” to spend more than $900 million from the federal American Rescue Plan Act. Even then, these programs won’t even be created or funded until late winter. They provide no immediate relief to struggling healthcare providers in Maine.
Despite the public harm which may result from massive public health and safety worker shortages wrought in the blind pursuit of 100% vaccination rates, the mandate has thus far survived judicial review. In a preliminary ruling issued October 13, Judge Jon D. Levy of Maine’s Federal District Court allowed Mills’ mandate to proceed, dealing a severe blow to a challenge from a group of healthcare workers. Plaintiffs’ appeals to the First Circuit Court in Boston and to the United States’ Supreme Court were swiftly denied, signaling that the Maine mandate is likely to be enforced. In denying appeal, the higher courts have acknowledged Judge Levy’s ruling as a sufficient review of the mandate.
A ruling in favor of the plaintiffs would have kept more nurses, EMTs, and other certified providers on the job; it would have spared hospital administrators from making tough choices to limit care, likely saving lives in the process. Hundreds of frontline care workers (many of whom worked through the height of the pandemic) now face termination for not taking one of the three available COVID-19 vaccines.
Legal observers might note that a judge in New York granted a preliminary injunction in a similar case challenging that state’s healthcare worker COVID vaccination mandate. An important difference between these two cases is that New York had removed religious and philosophical exemptions only for the COVID vaccines after the mandate had been effectuated. Maine law currently does not provide for religious or philosophical exemptions to any required vaccine since the passage of, and subsequent unsuccessful people’s veto effort to overturn, LD 798 from the 129th Maine Legislature.
Instead of requiring the state to meet the highest judicial standard of “strict scrutiny,” meaning it must show that it is using the “least restrictive means” to achieve a “compelling interest, ” Judge Levy in the Maine case determined the state’s action need only meet the lower standard of “rational basis” review because he regarded the mandate as both “neutral and generally applicable” and that “stopping the spread” of COVID-19 is a legitimate state interest. Mills and company did not contend that protecting hospital capacity, or even slowing the spread of the virus, was the reason for the mandate.
Levy, though, did “steel man” the plaintiffs’ arguments by simulating a review based on the more stringent level of “strict scrutiny.” Under this tact, Judge Levy considered the idea that the state’s vaccination mandate was the “least restrictive means” to accomplish its “compelling interest” in “stopping the spread” of COVID-19 in healthcare facilities.
He again concludes that mandating COVID-19 vaccination for employment in healthcare would meet the standard of strict scrutiny, but could more diverse scientific evidence have ultimately swayed him?
Levy constantly referenced the declaration filed by Dr. Nirav Shah, Maine CDC Director, in which he claimed that state data showed that “unvaccinated individuals are substantially more likely to contract COVID-19 and suffer serious medical consequences as a result,” and that “the percentage of COVID-19 outbreaks occurring in healthcare facilities is increasing rapidly and most of these outbreaks are caused by health workers bringing the virus into the facilities.”
Based on Shah’s testimony, the judge also wrote that a vaccination rate for healthcare facility staff under 90% is insufficient to “stem facility-based outbreaks.” The Maine Wire’s attempts to procure specific data from the Maine CDC on the relationship between healthcare worker vaccination status and outbreaks in those settings have not been fruitful.
It seems as though Judge Levy, like much of the Maine media, took Shah’s word without demanding any deeper scientific insight into his claims. It is reasonable for the judge to accept the state’s declarations of fact. After all, he should not have to also adjudicate a scientific debate within the context of a legal case, but when the scientific understanding of how we interact with SARS-CoV-2 and the vaccines is rapidly changing, greater scrutiny of the state’s take on the science is warranted.
Generally, Judge Levy accepted much of Shah’s declaration on its face, whether it be the unknown durability of natural immunity, the limits of a testing alternative to identify transmission, or whether widespread vaccination will reduce transmission of SARS-CoV-2 to the extent alleged by the state.
For example, Dr. Shah’s testimony contains an explanation of the concept of “herd immunity” which he defines as “an epidemiological phenomenon whereby even unvaccinated individuals are protected against an infectious disease by virtue of being in an environment with sufficiently high vaccination levels.” Curiously, Shah’s definition of “herd immunity” does not consider other ways in which a person could develop immunity to a disease, namely through surviving infection, which is traditionally how the concept was defined.
Before October 2020, the World Health Organization (WHO) described “herd immunity” as “the indirect protection from an infectious disease that happens when a population is immune either through vaccination or immunity developed through previous infection.” But this definition was changed in response to calls from the authors of the Great Barrington Declaration and others for a strategy that focused protection against COVID-19 on those most at risk. This idea was mistakenly branded by WHO as a “herd immunity strategy” in which proponents wanted to let the virus run its course throughout society without acting on it at all.
By using the WHO’s updated definition, Shah skirted around the idea that previous infection with SARS-CoV-2 imparts some level of immunity to the survivor and enabled Judge Levy to overlook this important aspect of the science in determining that the state could mandate a new vaccine on health care workers, even if they had gained natural immunity to the virus.
As part of his ruling, Judge Levy struck down every alternative to mandatory vaccination offered by the plaintiffs. Regarding a frequent testing alternative to vaccination, Levy again looks to Shah and writes, the “speed of delta transmission outpaces test-result availability” since PCR processing can take up to 3 days, a testing alternative “would require the use of rapid antigen tests,” which “are less accurate and in short supply.” For this reason, the judge did not see that testing would sufficiently fulfill the state’s objective. (page 32)
But, why wouldn’t testing be a sufficient alternative? In many ways, it is more reliable than vaccination status in determining whether a person is infected or contagious.
While false-negative rates for the prevailing rapid tests are worse for detecting asymptomatic infections of SARS-CoV-2, around 50% in those cases, they are about 80% effective at finding symptomatic infection. Given a prolific meta-analysis published in the Journal of the American Medical Association which found a low rate of asymptomatic transmission of COVID, this would seem like a reasonable accommodation to make, as opposed to firing hundreds of critical frontline workers.
Identifying where symptomatic infection exists, within 20 to 30 minutes with a rapid test, is an extremely valuable tool. One would think that with the enormity of federal and state resources spent on delivering the vaccines this year, a national scaling-up of rapid test production could be achieved as well.
A quick test in the moment can be a better predictor of someone potentially spreading the virus than their vaccination status. This July, the CDC identified that people infected with the Delta variant carry a similar viral load, whether vaccinated or not. This broadly means that they have similar capacity to transmit. Hardly a “pandemic of the unvaccinated.”
Prevailing studies and data from the US and abroad show that the available vaccines reduce the risk of severe illness and death from COVID-19. This is a public health success. What should give policymakers like Mills and Shah pause is the fact that more than one-in-nine COVID-19 cases since Mainers could become “fully vaccinated” (early January) have been breakthrough cases. Maine CDC notes in its data release that the “numbers likely reflect an undercount of the true number of breakthrough cases.”
Data collection on the COVID-19 vaccines, and the coronavirus pandemic broadly, has been difficult to procure from governments in the United States. Unfortunately, even without the proper evidence, public health officials will assume their policy works, promulgate it, and ask questions later.
In order to more fully assess claims that more vaccination means fewer cases and outbreaks, one must look across the pond. The United Kingdom Health Security Agency (UKHSA) publishes a robust vaccine surveillance report every week, tracking a 4-week period. The latest report shows that the observed rate of COVID-19 infection in “fully vaccinated” individuals ages 40 to 69 was nearly double between September 19 to October 17. In the last four reports, covering roughly mid August to mid October, observed rates of COVID-19 cases among fully vaccinated adults are the same, if not higher, than rates among those not vaccinated.

Is the UK data set a red herring or a canary in the coalmine? UKHSA warns that this data should be studied carefully because the rates can change with small differences in denominators; vaccine uptake varies with age. The report shows 20 to 40 year-olds have about 55-60% vaccine uptake, whereas more than 80% of the population 50 and older are vaccinated. Because older Britons are more likely to be fully vaccinated, it becomes difficult to compare a large sample to a small sample. Alas, the pattern is hard to ignore.
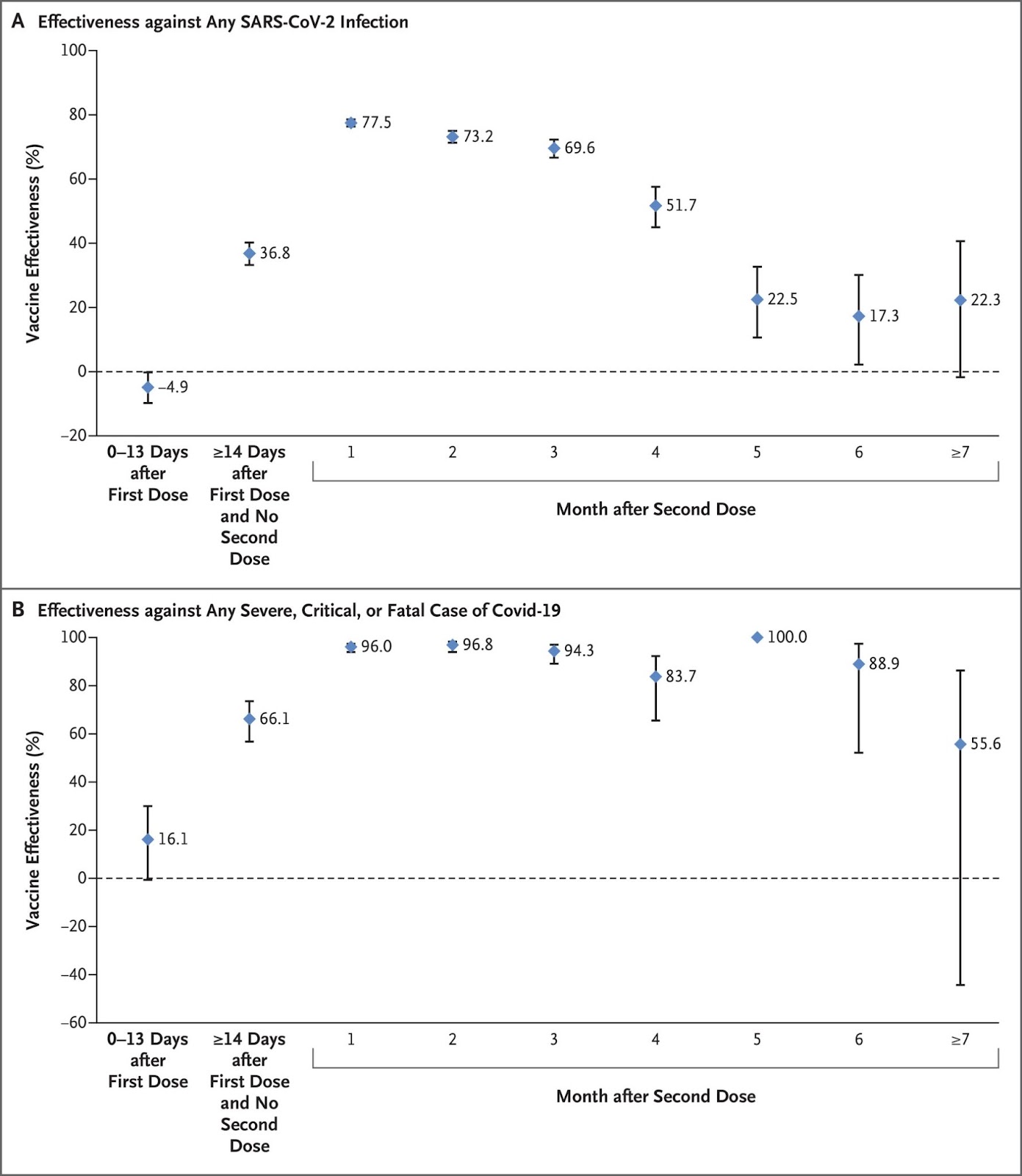
Other recent peer-reviewed studies have also cast doubt on long-term COVID vaccine effectiveness against infection. A recent study published in the prestigious New England Journal of Medicine in early October observed data from more than 900,000 Qatari citizens and found significantly waning effectiveness of the Pfizer product (BNT162b2) against infection. In addition to finding negative efficacy within the first 14 days of the first dose, researchers noted a significant decline in protection from infection “accelerating after the fourth month” to around 20% by five to seven months after the second dose. Observation stopped after seven months.
Mills, Shah and company like to say that “vaccines are our best tool to defeat the pandemic,” which is likely true as it relates to stopping preventable deaths among vulnerable adults. But unfortunately, it does not appear that universal vaccination will “stop the spread” of the virus that causes COVID-19, though it may slow it. The administration has compared this saga to polio and smallpox in order to rationalize its mandate, but current data on COVID vaccines show that they do not provide sterilizing immunity as do the polio and smallpox vaccines. Both smallpox and polio do not have any animal reservoirs; unlike SARS-CoV-2, they are only carried by humans. These factors made the global eradication of smallpox and the near-eradication of polio possible, and greatly distinguish those public health questions from the ones we face today.
Gov. Mills says that every person seeking care in Maine should know that their provider is vaccinated in order to ensure a standard of care. This is a talking point anchored in political science — cherry-picked studies and exploited public misunderstanding — not real science. The data show these individuals can catch and transmit the virus, even if vaccinated.
Shouldn’t a vaccine mandate, as the administration claims, be reasonably expected to keep those subjected to it from spreading the virus? Today, this is far from a guarantee; based on available data from across the globe, it is unlikely. And that’s why mandates are not the answer.