
Recently, labor shortages have been frequently reported across the nation, including in Maine and the New England region. A story in the Sun Journal on a shortage of psychiatrists in Maine noted that this issue extends to a lack of medical professionals as well. In the five years preceding the pandemic, Maine lost half of its licensed psychiatrists.
Lack of care in this area can lead to inadequate service for vulnerable people, and inflict additional stress on the primary care providers like physicians, nurse practitioners, or physician assistants who may prescribe medication but cannot fill the same clinical need as someone licensed to practice in the mental health field.
Like the pressures placed on working parents from a lack of child care, strained supply of skilled medical professionals has been a long-term trend for the Pine Tree State. Maine already has too few doctors, and the shortage is projected to become worse over the next several years. In 2020, Maine ranked last out of all 50 states for patient satisfaction of physicians.
Healthcare Needs Grow as the Population Ages
Demographic reports note an increasing workload for physicians as the state’s population continues to skew heavily toward older generations. Maine already claims the oldest median age of any state: more than 45 years old. The national median age is 38.4. It also has the highest share of the population aged 65 and older (21.2%) per the latest Census estimate. In 2016, the Maine State Economist estimated that the share of the population 65 and older will grow 37% by 2026.
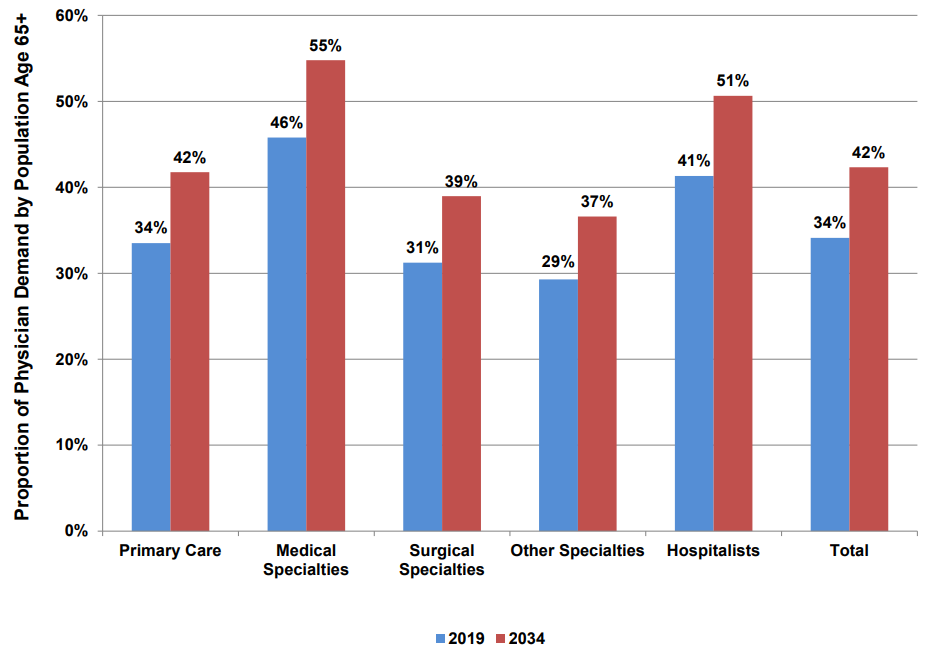
A higher share of medical costs are driven by older people, so as the population ages, demand for medical services rises. This means that even as the overall population remains relatively stagnant, Maine needs more practicing medical professionals per capita. The American Association of Medical Colleges (AAMC) anticipates a substantial increase in demand among patients 65 and older for physicians across the country: from 34% in 2019 to 42% in 2034.

AAMC also projects a national shortage of between 37,800 and 124,000 physicians by 2034. Researchers at The Robert Graham Center observed this trend locally in 2012, projecting that Maine would need 9% more primary care physicians (PCPs), a subset of total licensed Medical Doctors (MD) and Doctors of Osteopathy (DO), to meet expected needs. The Center’s follow-up report in 2018 found that the state had only gained 1.4% more PCPs since 2010.
Rural Areas Disproportionately Bear the Burden of Shortages
In addition to being the oldest state in the region, Maine is also one of the most rural. Thus, Maine faces yet another challenge in attracting enough medical professionals to the right areas to provide adequate healthcare. On a state-by-state level, Maine looks to be in fine shape compared to the region, but county-level data show a more dire picture, especially considering the rapidly aging population.
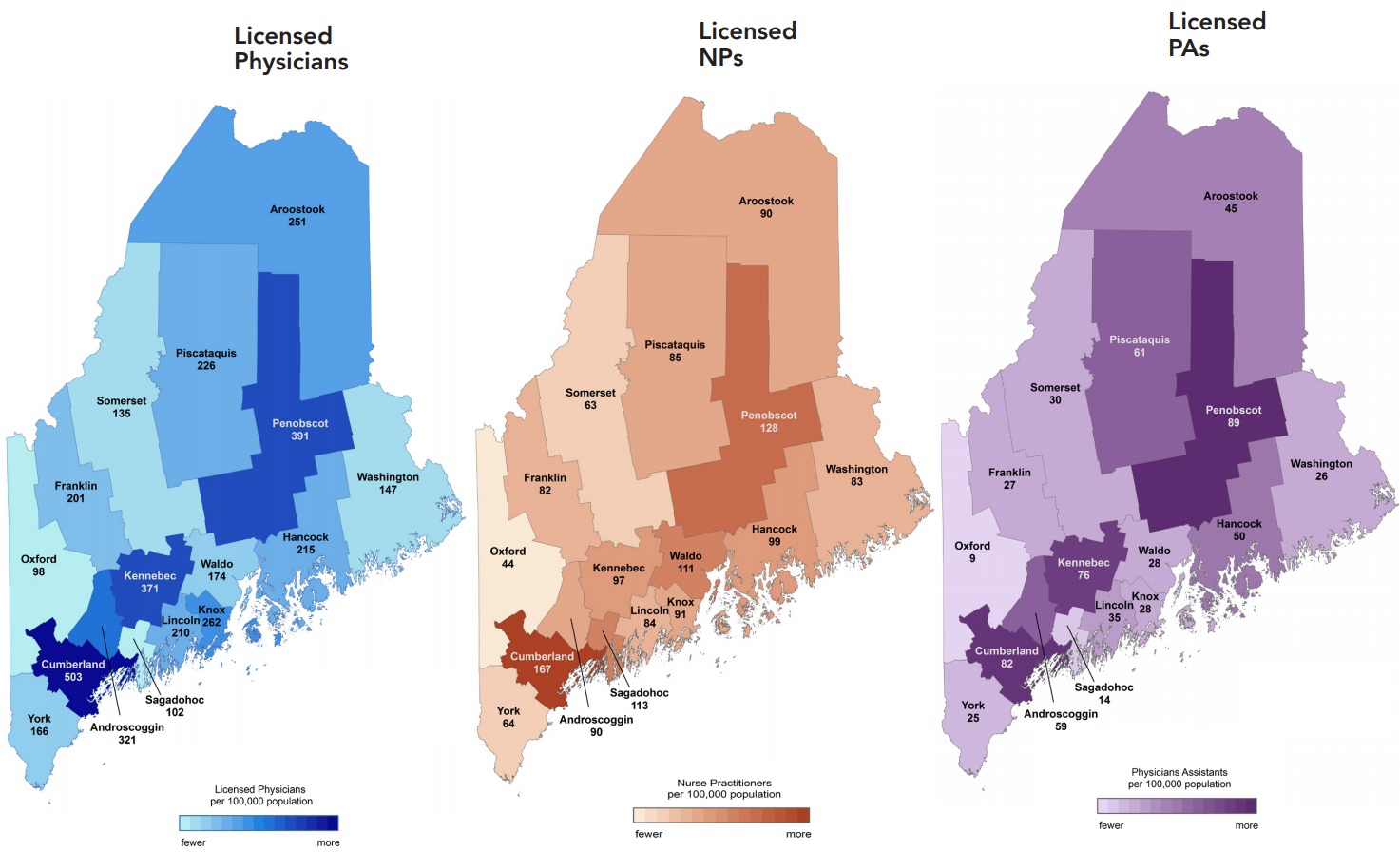
Researchers at the Center for Health Workforce Studies at the University of Washington (UW) noted significant geographic disparities in coverage in their 2019 report on Maine’s healthcare workforce. Counting MDs and DOs under the age of 75, the top four Maine counties (Cumberland, Androscoggin, Kennebec, and Penobscot) had an average of 396.5 physicians per 100,000 residents. By contrast, the bottom four counties (Oxford, Sagadahoc, Somerset, and Washington) averaged 120.5, less than one third the rate of the top counties.

Another pertinent question for anticipating future healthcare supply is how many currently-practicing physicians are approaching retirement age, and how that differs across the state.
The 2018 FSMB Census of Licensed Physicians in the United States counts physicians who are at least 60 years old as those likely approaching retirement. Maine has a higher share of physicians in this group than every state in the region but Vermont. Maine also has double the population and number of physicians of Vermont. The other four New England states’ share of older physicians is much closer to the national average of around 30%.
This disparity exists along rural/urban lines as well. A 2019 survey by the AAMC found that more than one-third of rural physicians in Maine are aged 60 or older.
The UW report noted that Maine’s physician workforce skews older, much like the national population. While only 28% of MDs and 40% of DOs licensed in Maine were age 44 or younger, “[h]alf or more of the physicians in many of Maine’s most rural counties were age 55 or older, indicating the potential for retirements to create gaps in future supply.” Midcoast and Downeast counties: Sagadahoc, Knox, Lincoln, Waldo, Hancock, and Washington had a 10-20% older physician workforce than Cumberland, Androscoggin, or Penobscot.
In the quest to attract younger doctors to rural Maine, there is good news: a study from the Center for Family Medicine showed significantly less burnout among family physicians in rural areas versus metropolitan or urban areas.
But, physicians are not the only piece of the puzzle. Attracting high-skill medical professionals extends to nurse practitioners (NPs) and physician assistants (PAs) as well. NPs and PAs generally have a narrower scope of practice than physicians. PAs may only practice under supervision of a physician but nurses may operate their own practice. Because of comparable service, and the lower threshold for entry into the NP field compared to physicians, care is often more cost effective through NPs. In Maine, the average nurse’s salary ($96,337) is nearly half that of the average physician ($177,302); both are at least 10% lower than their national averages. PAs in Maine make about the same as the national average ($107,500).
Between 2014 and 2018, Maine lost 2.2% of physicians, but gained 23.6% more NPs and 16.8% more PAs. Opportunities for cost savings by utilizing NPs or PAs could be a huge boon to Maine consumers, but geographical disparities in access to care persist among these providers as well.
Proposed Solutions to an Impending Shortage
Governor Mills recognizes this issue, and has proposed ways to address it in her upcoming spending packages. In addition to the state supplemental budget, which charts spending of newly-realized state tax revenue over the next two years, the governor is pushing another bill to spend the nearly $1 billion dollars in federal American Rescue Plan Act money sent to the state government. The governor refers to this bill as the Maine Jobs and Recovery Plan.
Under Part H of the spending bill, Mills proposes a new class of public-private partnerships to train hospital and nursing home workers known as the “Healthcare Workforce Initiative”. Recognizing that these shortages “affect Maine’s ability to attract talented workers since quality health care is often a priority for relocation,” Mills is offering a “pilot loan repayment program for certain health care professionals who commit to living and working in Maine for at least three years.” Qualified workers will be able to receive up to $25,000 per year and the lesser of $75,000 in aggregate and 50% of the recipient’s outstanding loan balance.”
While this could help ease the transition for some individuals from medical school into the field, will it close the significant gaps in coverage across the state? If workers are only on the hook to work in-state for three years in order to receive the bonus, how will this stem shortages anticipated over the next 10-15 years?
Research published in the journal Economic Development Quarterly in April 2020 found that these sorts of targeted, top-down industry incentives “crowd out other economic activity, potentially reducing long-term growth.” They also note that targeted tax and subsidy “incentives have a statistically significant, negative relationship with start-up rates.” This is a problem because, with fewer businesses overall, workers’ “job mobility” is limited. Ultimately, Mills’ workforce grant programs amount to little more than throwing money at a problem; gimmicks that distort market signals in the labor force, instead of tackling root causes of economic stagnation.
Another study of how incentives affect states’ fiscal health published in February 2020 looked at data from 32 states between 1990 and 2015. They found that “after controlling for the governmental, political, economic, and demographic characteristics of states, incentives draw resources away from states” and “negatively affect the overall fiscal health of states.”
Can Maine Compete?
NPs and PAs licensed to practice in Maine are also more likely to live in-state than physicians. The 2018 UW report found that 68% of physicians with Maine licenses had in-state addresses compared with 84% of NPs and 94% of PAs. A review of active MD licenses from June 10, 2021 found that only 57% are located in the state.
In 2018, 15.5% of U.S. physicians (210,334) held two active licenses; 6.6% (89,562) held three or more. The six states which make up the New England region recognized 79,840 active physicians’ licenses that year. How many of these multiple licensees live in New England?
Because of relatively high differences in income tax rates within a small geographic area, physicians may choose to reside in northern Massachusetts or southern New Hampshire instead of Maine, yet can easily access and serve their Maine patients. New England is a close-knit region where cross-border differences are often exploited by consumers; just look at overall tobacco sales since Massachusetts banned flavored products. Despite this abject policy failure, Maine Governor Janet Mills has proposed a similar policy in her supplemental budget.
Though it is not clear in data currently available, significant cross-state differences in income taxes (by multiple percentage points at the top rates) likely weigh in the minds of high-earning medical professionals licensed to practice in several New England states.
Perennial proposals in the Maine Legislature, like this session’s LD 498, a bill which would tax individual earnings above $200,000 per year an additional 3%, would not help attract more physicians to the state. If passed, Maine would have the fourth-highest top tax bracket in the nation, and the third-highest rate at the $200,000 income level, just behind California and Hawaii. Thankfully for prospective skilled medical professionals and other high-earning workers, LD 498 was voted down by the House on Wednesday.
Legislators should be wary of proposals to tax Mainers any further. Given the imminent shortage of advanced practice medical professionals in the state, we need to welcome doctors, not scare them away. While some might see practicing physicians as members of “the rich,” a 2019 survey found that almost 60% of doctors expect to spend at least six years paying off their medical school debt; a third expect to take at least 10 years. High income does not mean excess wealth.
Instead, lawmakers and Governor Mills should pursue the powerful combination of radically reforming state regulatory and tax policy to grow the number of skilled medical professionals in the state. Enacting universal licensing reciprocity and a repeal of Certificate of Need, with dramatic tax reform to lower individual and corporate tax rates, would help Maine be more competitive with our neighbors.
Since 2017, Maine has been a part of the Interstate Medical Licensing Compact (IMLC), a 33-jurisdiction agreement to streamline medical licensing, but the average Maine physician license still takes 45 to 90 days to process, versus 15 to 20 days for the average IMLC member state. While this and other consortiums like it are beneficial to lowering barriers to entry for doctors and nurses, there is clearly more progress to be made on speeding up Maine’s medical licensing process.
The state’s rapidly aging population, especially those dwelling in our most rural counties, would greatly benefit from an influx of medical professionals and facilities, driving competition and choice where there was little before. Public officials don’t have much time to address this systemic issue before it becomes a crisis of care.