
The rapid rollout of COVID-19 vaccination for young children is on the minds of nearly every parent in America today, but has American society fully answered the question posed to readers of the journal Toxicology Reports last quarter, “why are we vaccinating children against COVID-19?”
In just the first week, nearly one million children aged 5-11 received their first dose of the newly-emergency-use-authorized Pfizer vaccine for that population. More than 3,000 children in Maine received an injection within the first week, some in vaccination clinics stood up at their schools.
New data on pediatric vaccination rates from 19 states show a week after vaccines were authorized, 2.7% of kids ages 5-11 in these states have received their first dose. It's too early to read into statewide trends yet as the program continues to ramp up.https://t.co/B7NdMIFQKV pic.twitter.com/DHPbtk3RJC
— Benjy Renton (@bhrenton) November 11, 2021
When Pfizer announced that its childhood vaccine—a dose of mRNA one-third the size of the adult vaccine—mounted a strong antibody response in the trial group on September 20, it felt like a foregone conclusion that children would be lining up for COVID-19 vaccines in short order.
News reports leading up to the authorization amounted to little more than a copy-and-paste of that Pfizer press release, describing doctors and parents “eagerly awaiting” a COVID-19 vaccine for their children.
To the casual observer, it seemed that all that was necessary was to show that the vaccine works via antibody response, despite the broad recognition of waning immunity from the adult vaccines. Given that this vaccine is under an Emergency Use Authorization, are the risks to children from COVID-19 truly an emergency?
These stories were published despite the acknowledgement of fact that 5 to 11 year-olds face the lowest risk of death from COVID-19 out of any age group recorded by US CDC. Data presented to the Advisory Committee on Immunization Practices (ACIP) show a 0.44% hospitalization rate for 5-11 year-olds from COVID-19. It also noted a recorded 2,316 cases of multi-inflammatory system in children (MIS-C) and 94 deaths attributed to COVID-19 out of 1.9 million cases.
Is there any other age group with a lower COVID hospitalization rate than 5-11 year-olds?
— Nick Murray (@NickMurr) November 2, 2021
8,300/1.9 million = 0.44%
Maine CDC reports that just nine children aged 5-14 have been hospitalized for COVID-19 (0.086%) out of more than 10,000 cases among that age group, accounting for just 0.31% of the 2,900 Mainers hospitalized across the entire pandemic. Only 0.22% of Mainers under age 20 with a confirmed or probable case of COVID-19 have gone to the hospital.
Previous Maine Policy reports have covered the risks to children from the virus, including “long covid” related conditions. Available data to this question show that symptoms clear in more than 98% of children eight weeks after infection.
CDC data tell us that younger unvaccinated adults face a lower risk of COVID than older vaccinated adults. It makes sense that the same age-based risk differential would extend to the youngest among us, as the case trends from the pandemic have shown.
Even before the FDA’s Vaccines and Related Biological Products Committee (VRBPAC) and the CDC’s Advisory Committee on Immunization Practices (ACIP) met on October 26 and November 2-3, respectively, the White House and President Joe Biden rolled out their “operational planning” fact sheet. On October 20, Biden announced that the logistics of administering childhood EUA COVID-19 vaccines to nearly all of the 28 million children in the US would be ready, given eventual recommendation.
Children might not even need to be vaccinated for a disease for which they face rare severe outcomes. The vaccine itself could also carry potential risks for those who take it. These are all appropriate questions to ask when crafting a fully-fledged risk-benefit analysis, as the FDA and CDC were tasked to do. Especially if their recommendations will prompt various jurisdictions to mandate shots for children. Yet, questions on vaccine-related myocarditis (heart muscle inflammation) in mostly young males who had received the adult dose remain. These appropriate questions of safety were nearly completely absent from related news reports.
The heart risks have been known for months since CDC flagged myocarditis and pericarditis as notable adverse events (AEs) following COVID-19 vaccination. In August, the CDC published in its Morbidity and Mortality Weekly Report (MMWR) a breakdown of data pulled from the Vaccine Adverse Events Reporting System (VAERS) and found that nearly 10% of adverse reactions to the Pfizer shot from Americans aged 12 to 17 were severe adverse events (SAEs). Of those, 56% reported chest pain, 40% reported myocarditis, and 30% reported increased c-reactive protein, a signal for increased heart attack and stroke risk.
While VAERS cannot be considered a reliable data reporting system, it is the only official public clearinghouse for reporting vaccine-related adverse reactions. VAERS sends early-warning signals to scientists and public health officials at the CDC’s Vaccine Safety Datalink about which reactions need further study.
It is important to understand that anyone may submit a VAERS report, but medical providers are required by law to report any adverse event they believe to be related to vaccination to VAERS. As the CDC describes, “VAERS cannot determine if a vaccine caused an adverse event, but can determine if further investigation is needed.” Questions about the veracity of VAERS as a data source are valid, for the reason that it could contain a number of fraudulent reports. Yet, a Harvard Pilgrim report presented to The Agency for Healthcare Research and Quality at the US Department of Health and Human Services in 2010 estimated that “fewer than 1% of vaccine adverse events are reported.” The authors pointed to “a lack of clinician awareness, uncertainty about when and what to report, as well as the burdens of reporting: reporting is not part of clinicians’ usual workflow, takes time, and is duplicative.”
A preprint study from September conducted by Dr. Tracy Hoeg and colleagues found that children with at least one comorbidity have a higher risk from COVID-19 than from vaccine-induced myocarditis. For this population, vaccination looks reasonable, but this ratio is not the same for healthy children. The study also charted VAERS reports which met the CDC definition of a cardiac adverse event (CAE), and stratified that data by age. Authors estimated the case incidence of vaccine-induced CAEs to be between 94 and 162 per million children ages 12-17, for which the CDC estimates 66 per million.
In June, a member of the Vaccine Safety Team at CDC identified that 94-96% of patients reporting COVID-vaccine-related myocarditis were hospitalized within 120 days, the same standard used in the Hoeg pre-print study. Overall, Hoeg and colleagues found that boys aged 12 to 15 without medical comorbidities who received two doses of an mRNA COVID-19 vaccine were 3.7 to 6.1 times more likely to experience a vaccine-related CAE than to be admitted to the hospital for COVID-19 disease in a 120 day period.
These study participants were young but they received the adult dose with triple the mRNA than the childhood formulation, though much of the data available to FDA and CDC advisory committees stemmed from estimates like these.
A presentation to VRBPAC by Dr. Hong Yang, Senior Advisor for Risk-Benefit Assessment at the FDA’s Office of Biostatistics and Epidemiology, during the October 26 meeting showed considerable risks to young boys, even from the smaller-dose childhood jab. This data overlaid the risks for 12-17 onto several modeled scenarios for children 5-11.
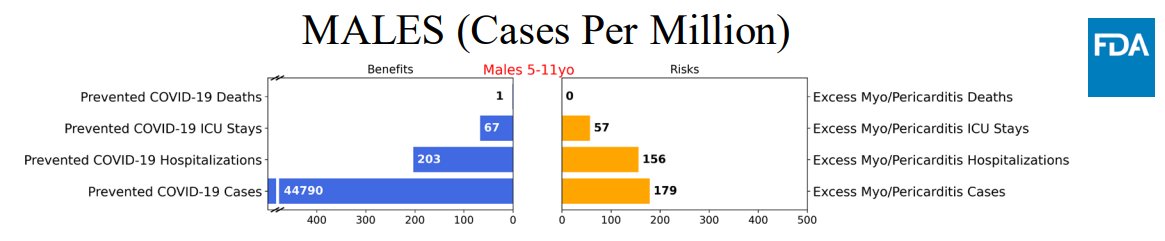
Shown in the graph above, Dr. Yang’s model predicted that vaccinating males aged 5 to 11 would prevent 67 ICU stays and 203 hospitalizations for COVID-19 per one million boys, but would also result in 57 ICU visits and 156 hospital stays for vaccine-induced myocarditis. This risk-benefit analysis only considered myocarditis and heart-related risks post-vaccination.
The low COVID-transmission scenario clearly showed no benefit in terms of hospitalizations. Shouldn’t the benefits of vaccination clearly outweigh the risks in every scenario?
They appear not to have corrected for over-ascertainment of COVID hospitalizations.
— Phil Kerpen (@kerpen) November 5, 2021
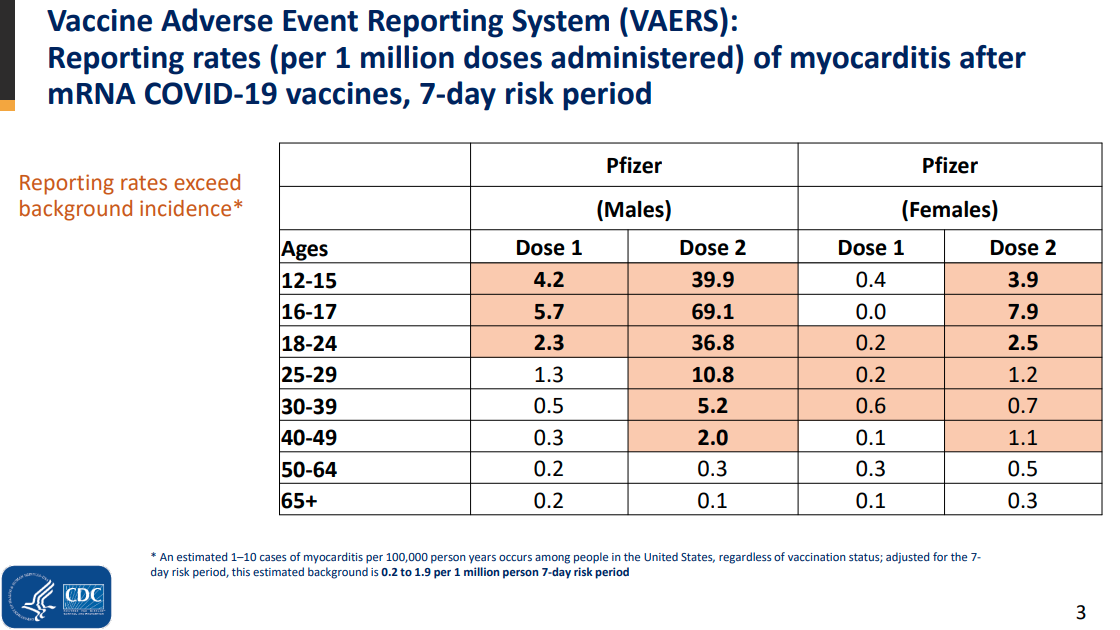
During the November 2nd ACIP meeting, Dr. Matthew Oster, a pediatric cardiologist and a member of the CDC’s Vaccine Tack Force, presented on “mRNA COVID-19 vaccine-associated myocarditis,” looking at the differences between different types of myocarditis and the related outcomes. He reported that, based on VAERS data, the rates of myocarditis reported within a 7-day risk period following mRNA vaccination were higher than the background rate, or what is assumed to occur in everyday life. Researchers estimate this rate to be between 0.2 and 1.9 cases per million. For those aged 12 to 18, vaccine-related myocarditis reports were many times greater for males than females, and in the case of males aged 16 to 17, reaching 30 to 300-times higher than the baseline.
Ultimately, ACIP gave final authorization to the childhood formula of Pfizer’s COVID-19 vaccine. That same day, CDC Director Rachelle Walensky endorsed the ACIP recommendation, allowing for the massive rollout witnessed in pharmacies, community centers, and even schools across the nation in the last few weeks.
In its final recommendation, CDC claimed that hospitalizations among children for COVID increased fivefold over the summer, but this statistic does not take into account a factor known for months, as reported in The Atlantic, that as much as one third of hospitalizations were misattributed.
Almost immediately upon CDC recommendation, the City of San Francisco moved to mandate all children receive the EUA Pfizer pediatric COVID-19 vaccine in order to attend schools in the city. This is puzzling, since many VRBPAC voting members noted after the vote that they wanted to provide parents the option to vaccinate their children. Credible scientists—such as Dr. Cody Meissner—noted their reluctance to endorse it due to the possibility that some institutions would mandate COVID-19 vaccination for young children because of their recommendation. Those concerns were quickly validated.
Without measurable benefit and yet-unknown potential risks, how can any scientific or public health professional recommend broad mandated COVID-19 vaccination of children? Even the FDA’s briefing documents for the VRBPAC meeting in late October recognized that the sample size of the prevailing Pfizer trial for its childhood vaccine “is too small to detect any potential risks of myocarditis associated with vaccination.” That risk won’t be truly known for years.
“Long-term safety of COVID-19 vaccine in participants 5 to <12 years of age will be studied in 5 post-authorization safety studies, including a 5-year follow-up study to evaluate long term sequelae of post-vaccination myocarditis/pericarditis.”
Maine CDC director Dr. Nirav Shah says he wants life “to be easier for your kid to be vaccinated than to be unvaccinated.” And the Mills administration’s policies will indeed make it easier, since vaccinated students will not have to quarantine and be removed from school upon exposure to someone who tests positive. No question that this policy does not adequately take safety concerns into account, but does it even match the current science on how vaccines affect transmission?
Given the current crop of vaccines and the characteristics of this particular coronavirus, mass vaccination does not look like the successful path it was once sold to be by public health officials. As many in the news media have begun to ask, why are the most heavily-vaccinated states (like Vermont and Maine) seeing the largest, most persistent cases and hospitalizations over the last few weeks, while other less-vaccinated states are not? This realization may be reaching the upper echelons of government, as a senior NIH bioethicist expressed concerns about mandating the currently available vaccines, saying that their current use is “extremely problematic.”
Based on what we know today, the available COVID-19 vaccines cannot “stop the spread,” especially since effectiveness of the Pfizer product wanes to 50% after 4 months and even less in months following, reaching near zero after just seven months. Indeed, this has fueled the push for additional “booster” doses, but where does this leave the newly-vaccinated school children 6 months from now?
Clearly, these significant concerns about vaccine effectiveness and the usefulness of mandates should extend to children. It may also be prudent to apply this principle to younger, healthy Americans whose immune systems are strong enough to fend off severe COVID-19 initially, as well as potential repeat infections. Hopefully, parents take the time to understand the risks and benefits to their children, because unfortunately, listening solely to media and state health officials will not ensure their consent will be fully informed.