

Covid Catastrophe Part III: What Emergency?
Covid Catastrophe is a seven part series examining the history of the COVID-19 pandemic, its impact on Maine and what data policymakers used to lock down society and centrally-plan our economy. Check back tomorrow for Part IV.
In Maine today, the spread of COVID-19 is largely under control. Indicators of disease spread, like infection rate, testing positivity rate, and R0 value, or “R-naught,” (the rate at which each infection leads to other successive infections), and indicators of outbreak severity, like case hospitalization rate and case fatality rate (CFR), have been on the decline since peaking in April and May. Although Governor Janet Mills has maintained the Civil State of Emergency originally declared in March, a review of current data shows that Maine is no longer in an emergency.
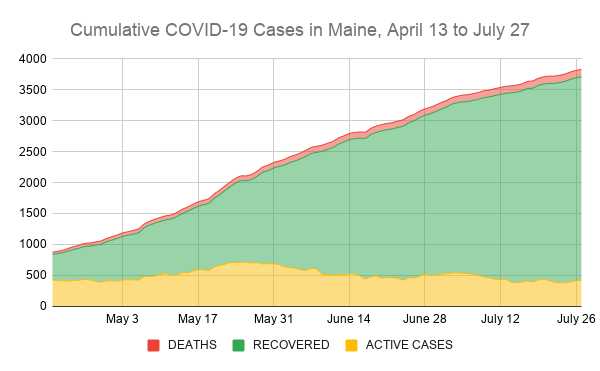
Today, Maine’s active case number hovers around 400, the lowest since early May. Although, sadly more than 120 Mainers have succumbed to the virus, current data shows a positive trend given the recent dramatic increase in tests administered since late May. Upon a cursory observation of daily media reports on state CDC briefings, the average observer would not see this as a measure of progress. The public is much more likely to hear total, cumulative case numbers more prominently stated, without mention of the progress of active cases, hospitalizations, or testing rate, leaving the layman to believe that the virus is still spreading rapidly throughout the state.
Current case data show that the virus is under control in Maine. The rolling 7-day average of positive coronavirus tests has dropped below 1%, the overall testing rate is dipping below 3%, hospitalizations have declined to about a dozen, and our fatality rate (CFR) is just above 3%. This is still significantly higher than studies conducted worldwide that estimate between 0.5-1% CFR. This could be attributed to the still-inadequate level of testing needed to find all active cases, the tendency of those with mild symptoms to forgo testing, as well as the unresolved scientific accuracy of active virus tests and antibody tests.
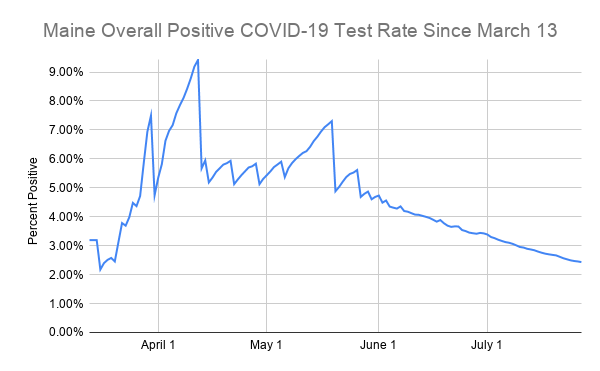
Maine’s R0 for COVID-19 is now below one. This means that fewer than one person will become infected for every currently infected person, signifying a slowing spread of an outbreak. The R0 has fluctuated between 1 and 1.2 for the vast majority of the spring, since state CDC testing data was comprehensive enough to provide a reasonably accurate representation of case distribution. This has led to significant decreases in numbers of new cases, hospitalizations, and the state testing positivity rate, a key metric that Dr. Nirav Shah, director of the Maine CDC, consistently referenced as an indication of the degree of danger to Maine people from the outbreak

The two figures of Maine, one by county and one by ZIP code, demonstrate the overall distribution of confirmed and probable cases of COVID-19 across the state as of July 21. Early on in the pandemic, observers and public health officials noticed that population density played a large role in determining how quickly the virus could spread. This was part of the rationale behind “stay at home orders” and limiting “non-essential” travel and commerce: to decrease the amount of close interactions among the population.
As New England states go, Maine is exceptionally well-suited to weather a new outbreak if the priorities of state officials are fine-tuned. The sparse population, combined with vast geographical distribution of at least two-thirds of the state’s land mass, contributed to significantly limited spread of the virus. For instance, Cumberland County, with the largest share of cases by far and over 50% of the state’s total COVID-19 deaths, contains 330 people per square mile. The City of Portland, at over 3,000 people per square mile, has recorded over 800 cases within its three ZIP codes, almost 40% of the total caseload in the county.
By contrast, Aroostook County contains under 11 people per square mile, and in Piscataquis County, just 4.4 people per square mile. Regional differences across the state vary significantly, yet for over two months, the state government treated the entire state as an emergency zone, neglecting to balance these differences with the potential devastation of Mainers’ livelihoods. It was not until May that the Mills administration attempted to parse out these differences with its “Rural Reopening” plan.
In Maine, and in New England broadly, deaths and hospitalizations due to COVID-19 are stabilizing. The fact that we are seeing a more even distribution of cases by age may be an encouraging sign because we are beginning to understand the breadth of different experiences people have when encountering this new virus. It further highlights the fact that those most at risk of death are the elderly.
Although slightly more than half of cases are Mainers aged 70 and older, they have made up nearly 85% of fatalities.

Rising COVID-19 case numbers in Maine and across the United States during the recent summer months, now added to the case totals, are showing a broader age distribution. That is to say, more people between the ages of 20 and 50 are being confirmed to have contracted the new coronavirus. Beforehand, the vast majority of cases were from those over 65, a group much more likely to experience a severe case, seek care, and be hospitalized. The effect that this sort of selection bias would have on the currently available data is just beginning to be realized.
It is possible that institutions from the CDC, WHO, and Maine state government miscalculated the date at which the new coronavirus reached U.S. shores, and therefore how many Americans could have been infected or even exposed to the virus this year. Recent reports showing outlier “influenza-like symptoms” at Maine hospitals as early as mid-January suggest that the coronavirus may have been in Maine many weeks before the state shut down economic activity in an attempt to stem the spread.
Data released by the CDC on July 21 estimated that current figures on how many Americans could have the coronavirus are 10-13 times less than what was previously understood. The authors attributed this estimation to the possibility that many people who had mild or no illness and did not seek medical attention, yet still carried the virus, “may have contributed to ongoing virus transmission in the population.” Considering that surveys across the globe show that mild or asymptomatic cases of COVID-19 exist in anywhere between 20-35% of those infected, these reports likely gets us closer to understanding the true spread of the disease among the population.
Overall, this data should give Americans hope that we are getting closer to meeting the threshold of herd immunity. Herd immunity is the idea that once a substantial portion of a society has accumulated antibodies from being exposed to a new virus, spread of the virus slows and the vulnerable and immunocompromised are protected from infection. While the adequate level of exposure to the coronavirus to trigger herd immunity is currently unknown, this might be our quickest way out of this crisis, considering new vaccine development is a lengthy endeavor.